
While it’s beyond the scope of a blog post to present a thorough discussion of vulvar and vaginal anatomy, some explanation is necessary to understand the procedures most patients seek. Following is a brief overview of the female anatomy and why a woman may desire to seek genetic plastic or cosmetic surgery.
A Brief Anatomy Lesson
The labia majora and labia minora in women act as “guardians of the vaginal opening.” The former are wide cushions analogous to the male scrotum; the latter, which are formed as side-by-side folds descending down from the clitoral hood, act as “curtains” for the vaginal opening (called the “introitus”).
The upper portions of the labia minora begin as one or several folds descending down from the different parts of the clitoral hood. The frenulum (the fold that descends down from the clitoral head or “glans”) joins the upper fold(s), curtaining the edge of the introitus. The labia minora can end just above the base of the vaginal opening, but sometimes it continues over to the other side or descends down onto the perineum as the “fourchette” or “posterior commisure.”
That’s a lot of medical terminology thrown at you all at once, so here’s a diagram to make it easier to understand:
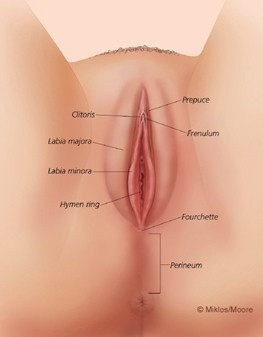
Vulvar Anatomy. Courtesy of John Miklos MD and Robert Moore MD of Atlanta Urogynecology Associates. Used with permission.
When standing, many women’s labia minora are tucked away and not visible from above. Protrusion beyond the labia majora (the outer, wider and more “puffy” lips) while standing is often a cause of significant concern to women.
Likewise, the outer lips (the labia majora) may become enlarged, redundant or “droopy” and be a source of cosmetic dissatisfaction. This especially occurs with childbirth and aging.
The labia majora and outer surfaces of the labia minora consist of a skin-type covering over loose fibro-connective tissue. The labia minora contain sensitive nerve fibers, especially in the uppermost portion where the hood and frenulum come down to form the top-most portion of the minora. During sexual arousal, they become engorged and contribute to erotic sensation and pleasure.1
Changes Over Time
There is a wide range of normality when it comes to the labia. As in women’s breasts, where “normal” can include everything from an AA to an EE cup, women’s labia come in a wondrous array of shapes and sizes.
Attempts have been made to define “normal” as it relates to labial size, but this is admittedly difficult to do. Defining exactly where to measure from, and how much to “stretch” (or not stretch) this elastic tissue, has not been satisfactorily defined. In addition, even if a body part is considered to be “within the normal range,” it does not automatically follow that its form or function is satisfactory to its “wearer.”
It’s important to note that, although there are several reoccurring anatomic “types,” I have never seen two women’s labia that look exactly alike—or, for that matter, two sides of the same woman that exactly “match.” There is such a wide range of normality.
As time goes by, the vulva and vagina undergo several anatomic changes, including vaginal laxity, as they are weakened or stretched by age and/or childbirth. Aided by genetic predisposition, obstetrical forces (especially large fetuses), a long hard push and, eventually, age, the upper vagina may widen, and even the bladder can lose its fibromuscular support and herniate downward, pushing into the vagina and beyond. The rectum can also bulge into the vagina, and portions of vaginal skin push its way outward. In addition to obvious challenges to urinary continence and the ability to evacuate stool, these various “pelvic relaxations” often impact a woman’s sexual function.2
The processes of pregnancy and childbirth involve major adaptations of the vagina and pelvic floor to allow the opening necessary for childbirth and then later return to a near prepregnant state. Frequently, this recovery process is incomplete and can lead to feelings of “looseness” and diminished “grip-ability.” These all have their consequences in the sexual arena.
A combination of childbirth(s), big babies, tough deliveries and genetics often conspire to stretch, relax and break down the muscular and fibrous supports of the vaginal wall. The result: a widened vagina and loss of the natural downward tilt, resulting in much less penile pressure, especially on the clitoris/anterior wall. This can lead to less powerful orgasms or difficulty attaining orgasm in the first place.3
Patients Say It Best
So, why on earth would an individual woman desire to undergo surgery in this intimate and sensitive area? What would lead her to consider this, much less discuss it with a healthcare practitioner she hardly knows?
Patients’ rationale is real, and compelling. Actual quotes from women I’ve helped say it best:
“When you feel bad about your body, especially this part of your body, it’s kind of impossible to let your true feelings and passions show.”
“I was very, very self-conscious about the way I looked. Now I feel free. I just feel normal. I have nothing to hide.”
“I just felt that I keep myself in shape everywhere else… [The surgery] has given me more intense sexual enjoyment.”
“It never bothered my husband, but it was always like ‘Yuck!’ All I know is that what I had, I didn’t like.”
My experiences after over 15 years of providing genital plastic services for women parallel those of other experienced surgeons. Women requesting alteration of their labia and/or clitoral hoods do so for either cosmetic/self-esteem or functional reasons:
- “I feel self-conscious.”
- “I don’t want to do it with the lights on.”
- “I’m so much bigger than everyone else.”
- “I don’t like those flaps sticking out between my outer lips when I stand; it’s gross.”
- “I just don’t like how I look.”
The majority of women requesting alteration also note functional problems: chaffing with jeans and other tight clothing, self-consciousness when wearing thong underwear or bathing suits, discomfort exercising (especially bike riding), painful sex, hygiene difficulties, deviation or “splashing” of the urinary stream hitting the labia, and the frequent need to “rearrange” oneself.
Women requesting a vaginal tightening operation often feel their labia are large and bothersome to them and request surgeries for both. Women who come to see me inquiring about vaginal tightening rarely come in at the urging of their sexual partner, although the majority of the time they have discussed their concerns with their partner (if they have one).
These women are quite clear as to whose benefit they are considering surgery: their own. They tell me that sex is “not the same,” that they experience less friction, less pressure and often less arousal. Women frequently comment that, since childbirth(s) and with age, it takes them longer to climax and they find their orgasms are less powerful. They “feel loose” or have the “sensation of a wide vagina.” Although they may still experience “clitoral orgasms,” their more robust “vaginal orgasm” no longer occurs. And though there are typically cosmetic issues with the appearance of the vaginal opening, this is always secondary to their functional, friction and orgasmic issues.
These decisions are not hastily made. Women requesting genital revisions are, for the most part, a well-educated group. The average woman I see for labiaplasty has felt she was “larger” for several years but wasn’t aware that anything could be done until recently. Many patients who consult with me have been considering surgery for an average of 2-5 years. They have visited several websites, and many have gone to their family physician or their OB/GYN but have been rebuffed (“you don’t need to do that…”) by health care providers who are less than savvy in regards to the significant psychological and psycho-sexual toll these real or perceived anatomical situations take on individuals.
Excerpted from Dr. Goodman’s Ebook Everything You Ever Wanted to Know About Women’s Genital Plastic & Cosmetic Surgery.
1. The anatomy of the distal vagina: towards unity. Journal of Sexual Medicine 2008 H.E. O’Connell, N. Eizenberg, M Rahman, J. Cleeve,.
2. Hypertrophy of the labia minora; experience with 163 reductions American Journal of Obstetrics and Gynecology 2000 R Rouzier, C Louis-Sylvestre, BJ Paniel, and B Haddad
3. Female orgasm(s): One, two, several. J Sex Med, 2012. EA Jannini, A Rubio- Casillas, B Whipple, O Buisson, BR Komisaruk and S Brody.